The Ditch We Wound Up In

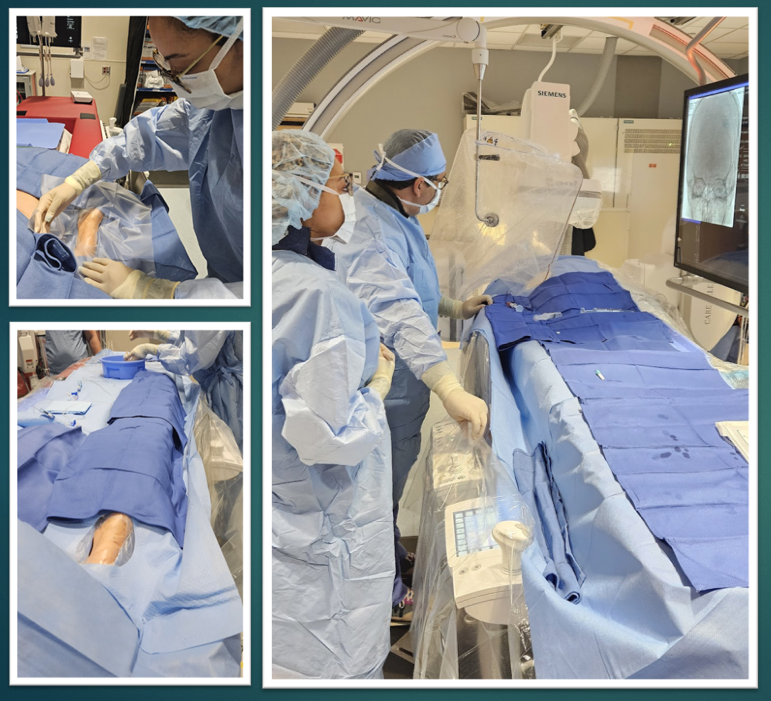
A common sight in the Cath lab and IR, the radial ditch
Radial access changed where we work. Nobody had a solution beyond the wrist.
When radial access took over the IR and cath lab, patients and most providers celebrated — and rightfully so. Fewer bleeding complications. Earlier ambulation. Better patient outcomes. The wrist replaced the groin as the preferred access site for a huge portion of interventional procedures, and that was a win for everyone in the room.
But something got left behind in the excitement.
There's been a lot of conversation about radial access over the years — the learning curve, hand supination, how to position the arm. Manufacturers rushed to design arm boards with supination cradles. Straps got more sophisticated. Wrist positioning became a topic at conferences. Those are real challenges, and the industry was right to take them seriously. Getting the hand positioned correctly matters.
But what almost never came up is what happens from the wrist distally, going toward the foot end of the table.
There's a gap there. A trough. A gully. A ditch — call it what you want, we all have a name for it — and it's one of the most underappreciated workflow problems in cath and IR labs today.

Arm positioning is important, but optimizing the physician workspace is paramount
"Radial access changed where we work. Nobody had a solution beyond the wrist."
Think about what's happening in that space during a complex intervention. You have coaxial systems, Monorail systems, triaxial systems. Long wires running off the wrist and dropping into dead air before they hit anything solid. That drop creates the potential for gravity to do its thing. Redundancy is energy — for better or worse — and when there's nothing supporting that slack, it can result in unwanted movement inside the patient's body. That's not a minor inconvenience. That's a patient safety concern.
The problem isn't only how to supinate the hand. Wrist positioning is a genuine challenge — one the industry has at least tried to address. But the ditch is a bigger problem, and almost nobody has touched it. We adapted to radial. We learned the setups, adjusted our workflows, and figured out how to keep the arm where it needed to be. What we couldn't fix with creativity and folded towels was the dead zone between the wrist and the operator — that stretch of unsupported space where catheters sag, wires go slack, and the physician has to compensate with their body every single time.
We spent years refining the access conversation and almost no time asking a simpler question: what does the operator actually need between their hands and the patient? The answer isn't another strap. It isn't a fancier supination cradle. It's a continuous, stable surface — something that eliminates the ditch entirely, gives wires and catheters somewhere to live, and creates a consistent interface between the physician's body and the patient from the wrist all the way through.
Not a patchwork of workarounds that gets rebuilt differently every case. Not a setup that works for one operator but falls apart for the next. A real solution — one that treats the operator's workspace with the same seriousness we've always given the access site itself.

Case set up can vary from operator to operator. The example above may prove difficult for the physician in a prolonged procedure
The shift to radial was one of the best advancements in a generation. The workspace around it deserves to finally catch up. Request a consultation with a Stratus Clinical Specialist to see if V.I.S. might be a good fit for your lab. Visit our Contact page today!
Stratus VIS allows for a flat runway from the wrist, to the end of the table

Stratus VIS benefits the physician and assistant with the ability to use lateral pop-in shields that are often abandoned due to obstruction to the access site. VIS solves this problem by bringing the working height to the optimal level
